
Ed Ritvo is a major figure in autism research. For decades, he and his colleagues explored the anatomy and physiology of children diagnosed with autism. In Understanding the Nature of Autism and Asperger’s Disorder, published in 2006, Ritvo sets out their key findings:
-stepwise rather than smooth, developmental trajectory
-perceptual inconstancy
-delayed language development
-delayed development of relatedness
-delayed maturation of REM sleep
-delayed development of balance system
-multiple differences in brain anatomy and function.
Despite the breadth and detail of their research, many findings were inconclusive because some, but not all, participants showed particular features. Ritvo concluded that new tools, notably gene research, were required before the causes of autism could be identified.
On re-reading Ritvo’s book recently I noticed things I’d overlooked first time around.
- Bleuler wasn’t an historical figure to Kanner or Asperger
In Chapter 1, Ritvo introduces us to the to the eminent Chester Keefer, Dean of the Boston School of Medicine when Ritvo trained there in the 1950s. Dr Keefer insisted his medical students study the history of a medical condition. Ritvo notes that Leo Kanner, who published his seminal paper ‘Autistic disturbances of affective contact’ in 1943, shared with Keefer “a love for the history of medicine and the wisdom it conveyed. This is why I am sure that Dr Kanner was very familiar with the writings of a famous Swiss psychiatrist, Eugen Bleuler. This is because he borrowed Bleuler’s term “autistic”: to describe the fact that his young patients could not relate emotionally to others.” (p.21). Ritvo makes the same claim for Hans Asperger (p.23).
But Kanner and Asperger wouldn’t have had to go far back in history to borrow Bleuler’s term ‘autistic’. Bleuler, based in Zurich, coined the term ‘autism’ to describe a feature of schizophrenia in his Dementia Praecox, oder Gruppe der Schizophrenien (Dementia Praecox, or the Group of Schizophrenias) published in 1911. His much reprinted Lehrbuch der Psychiatrie (Textbook of Psychiatry) came out in 1916, only five years before Leo Kanner qualified in medicine in Berlin, and 15 years before Asperger qualified in Vienna. In other words, Bleuler was as much of an historical figure to Kanner and Asperger as Chester Keefer would have been for Ritvo. Kanner and Asperger used the term ‘autistic’ in the way it was used in contemporary textbooks. The fact that Ritvo thinks Kanner and Asperger viewed Bleuler as an historical figure implies that he wasn’t aware they were contemporaries.
- Ritvo’s medical model is incomplete
Ritvo also introduces us to Chester Keefer’s medical model of disease (p.18).

Ritvo is writing for a non-specialist readership, so might have simplified the model. But it omits some important features.
Symptoms: what the patient reports. Signs, in contrast, are features of the condition that can be observed by others. Autism has always been diagnosed on the basis of signs rather than symptoms, but Ritvo doesn’t include signs.
Pathology: what we think of as abnormal or pathological depends on what we think normal is. There is no standard issue human being. Variation between human beings isn’t always pathological. Autistic characteristics aren’t always pathological.
Causes: A particular pathology can be due to one or more causes, but similar symptoms can result from different pathologies. There’s no doubt that everyone with a fever, sore throat and rash has a sore throat, fever and rash. But those symptoms could be caused by smallpox, chicken pox or measles, to name but three. There can be different causes for similar symptoms in different patients. Similarly there can be different causes in different people for autistic characteristics.
- Turning an adjective into a noun isn’t just a quirk of language
Ritvo comments: “We have a tendency in our language to change adjectives into nouns. Thus, soon after Dr Kanner’s first paper appeared with the adjective “autistic” in the title, it quickly morphed into “autism”: a thing. Now children had autism or were called autistic” (p.21). Ritvo attributes autistic [adjective] turning into autism [noun] to a tendency of language. In fact, it’s a cognitive process known as reification (making into a thing). Here’s how the transformation from ‘autistic’ to ‘autism’ appears to have happened:
Eugen Bleuler used der autismus [noun] as a descriptive shorthand term for one of the characteristics shown by schizophrenic patients. Medicine is replete with shorthand descriptive nouns because physicians observing patients need to make notes quickly.
Let’s say a patient shows dysphasia (difficulty with speech) and alexia (inability to read). You could say that they ‘have’ dysphasia and alexia. But they don’t ‘have’ dysphasia and alexia in the same way as people ‘have’ measles or malaria. Measles and malaria are specific medical conditions with known causes, so the diagnosis tells you what the signs, symptoms and causes are. In contrast, dysphasia and alexia are merely descriptive labels. They could be caused by a stroke, a tumour or traumatic head injury; the labels don’t tell us.
Bleuler coined the term autism as merely a descriptive label. Kanner’s 1943 paper was entitled ‘Autistic disturbances of affective contact’ because Kanner was using autistic [adjective] to highlight similarities between his child patients and one of the features of Bleuler’s schizophrenia (some of Kanner’s patients had previously been given a diagnosis of schizophrenia).
It’s true that by 1956, Kanner and his colleague Leon Eisenberg (Eisenberg & Kanner, 1956) were no longer referring to “autistic [adjective] disturbances of affective contact”, but instead to “infantile autism [noun]”, but that wasn’t due to a tendency in English to change adjectives into nouns. It was because Eisenberg and Kanner felt there was sufficient evidence to support Kanner’s original hypothesis that he had identified a “unique ‘syndrome’, not heretofore reported” (Kanner, 1943 p.242).
That would have been a reasonable conclusion had it not been reached by drastically reducing and broadening the number of “essential common characteristics” exhibited by the children. Kanner had originally described 20 very specific “essential common characteristics” in 11 children – which Kanner’s own observations showed were neither essential nor common. By 1956, 120 children had been diagnosed with Kanner’s syndrome, but some of Kanner’s original ‘essential common characteristics’ had been discarded, and the remaining 15 were collapsed into five. And in the 1970s, Lorna Wing and Judith Gould (Wing & Gould, 1979) screened nearly 1000 children and reduced the number of criteria to three (later known as the Triad of Impairments).
What is autism anyway?
In short, the larger number of children diagnosed, the fewer and broader the diagnostic criteria had become. Or to put it another way, broadening the diagnostic criteria meant that more children qualified for the diagnosis. It’s the equivalent of diagnosing all patients with a fever, sore throat and rash as having ‘fever-sorethroat-rash’ disease even if each patient has a distinctive rash indicating smallpox, chicken pox, or measles. ‘Autism’ or ‘autistic’ as descriptive shorthand labels had been reified into a thing called ‘autism’.
Why does it matter if Ritvo thought Kanner and Asperger saw Bleuler as an historical figure, or that he thought ‘autistic’ had morphed into ’autism’ due to a quirk of language? It matters because our conceptual model of a medical condition affects the way we interpret data about the condition.
‘Autism’ is a broad label. Many different underlying physical variations can result in autistic characteristics (see for example The Biology of the Autistic Syndromes by Gilberg & Coleman). But practitioners are pretty much obliged to use the official (broad) diagnostic criteria for diagnosis or accessing support. So are researchers, if they want to qualify for funding. This means there’s an assumption implicit in their research models, that all the people in an autistic group will have the same cause for their autistic characteristics. Here’s a hypothetical example to illustrate the type of problem that causes (please note this is a made-up experiment and I’ve simplified the representations of the results to illustrate the point)…
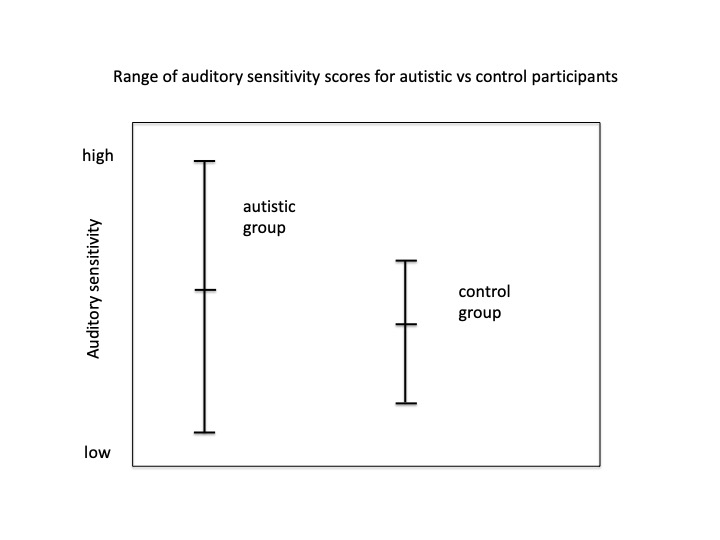
Many people diagnosed with autism report being hypersensitive to sensory stimuli (visual, auditory, tactile etc). Let’s say we design a series of experiments to test the hypothesis that autism is caused by sensory hypersensitivity. We might start by comparing auditory sensitivity in an experimental group of 20 people diagnosed with autism, and a control group of 20 typically developing people.
Let’s also say our results show that on average, our autistic group have higher scores for auditory sensitivity than our control group, but the difference isn’t statistically significant. We could represent the mean scores like this:

Furthermore, two members of the autistic group have the lowest auditory sensitivity scores of all participants, and three of the control group have higher scores than the autistic group average.
What do we do with the atypical scores in both groups? If we include them in our data we get an inconclusive outcome, but if we assume they’re due to an experimental artefact, call them ‘outliers’ and ignore them, our average scores will be statistically significantly different.
Alternatively, we could further investigate the variation within both groups, because:
-We might actually have two groups of autistic people – one where auditory hypersensitivity contributed to their autism, and one where it didn’t, or
-Auditory hypersensitivity might vary across the general population and be incidental to a diagnosis of autism.
Our example is a made-up experiment, but similar results have been found in real experiments (Gerrard & Rugg, 2009). Inconclusive findings about x being a cause of autism, are usually interpreted as ‘there is no evidence of x causing autism’ which is further interpreted as ‘x doesn’t cause autism’. Of course absence of evidence isn’t evidence of absence, especially if the absence of evidence is due to groups of people diagnosed with autism being assumed to be homogeneous rather than heterogeneous.
Ritvo pioneered some important research, but progress in much of it stalled solely because of the assumption in the research design that people with autistic characteristics form a homogeneous group. The later genetic studies,that Ritvo was looking forward to, have made it clear that different people can have different causes for their autism.
References
Gerrard, S & Rugg, G (2009). Sensory Impairments and Autism: A Re-Examination of Causal Modelling, Journal of Autism and Developmental Disorders, 39,1449-63.
Gillberg, C & Coleman, M (1992). The Biology of the Autistic Syndromes (2nd edition). Mac Keith Press.
Kanner, L. (1943). Autistic disturbances of affective contact. Nervous Child, 2, 217-250.
Ritvo, E R (2006). Understanding the Nature of Autism and Asperger’s Disorder, Jessica Kingsley Publishers.
Wing, L. & Gould, J. (1979). Severe impairments of social interaction and associated abnormalities in children: Epidemiology and classification, Journal of Autism and Childhood Schizophrenia, 9, 11-29.

